CIN 3: severe abnormalities
CIN 3 means severe abnormalities. Treatment by the gynecologist is necessary. This is still a precancerous stage, not cancer, but it is important to act now.
What is CIN 3?
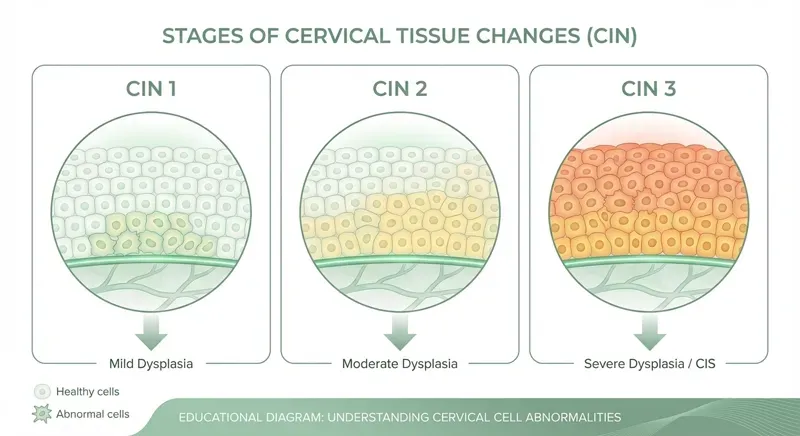
CIN 3 (Cervical Intraepithelial Neoplasia grade 3) means that the entire epithelium, all cell layers of the cervical mucosa, contains abnormal cells. The abnormalities are severe and involve the full thickness of the tissue.
Important: CIN 3 is still not cancer. The abnormal cells have not broken through the basement membrane, which is the border between the superficial tissue and the deeper connective tissue. However, CIN 3 is considered a direct precursor to cervical cancer. Without treatment, an estimated 30-50% of CIN 3 cases develop into cervical cancer over a period of years.
Therefore, treatment for CIN 3 is necessary. A watchful waiting approach is not a responsible option with this diagnosis.
CIN 3 is a severe precancerous stage, but it is highly treatable. After a successful LEEP procedure or conization, the prognosis is excellent. Early treatment prevents progression to cancer.
The treatment process for CIN 3
With CIN 3, the gynecologist will always advise treatment. The standard treatment is a LEEP procedure (LEEP/LLETZ) or a conization. During a LEEP procedure, a portion of the cervix is removed using an electrical loop. With a conization, a cone-shaped piece of tissue is removed. This is a more extensive procedure used when the abnormalities are deeper.
The standard medical process for CIN 3
Colposcopy and biopsy
The gynecologist confirms the diagnosis via colposcopy (magnifying glass) and biopsy (tissue examination). The biopsy determines the CIN grade.
LEEP procedure or conization
The abnormal tissue is removed. The procedure takes approximately 15-30 minutes and is performed under local anesthesia. The removed tissue is sent for pathology examination.
Pathology results
After 2-3 weeks you will receive the results: are the surgical margins clear? Is there any invasive growth? This determines the follow-up policy.
First check-up after 6 months
Smear test and HPV test to check if the abnormalities have been completely removed and the HPV virus has been cleared.
Long-term follow-up
Annual checks for at least 5 years. With CIN 3, the risk of recurrence is higher than with CIN 1 or CIN 2.
The effectiveness of a LEEP procedure for CIN 3 is high: in about 75-90% of women, the abnormal cells are successfully removed. But there is an important caveat: the HPV virus and the abnormal cells are not always removed.
The role of HPV Health in CIN 3, honest and transparent
We want to be very clear here: gynecological treatment is necessary for CIN 3. Escharotic treatment is not an alternative to a LEEP procedure or conization for CIN 3. This is a situation where conventional medicine provides the correct and necessary treatment.
What HPV Health can offer for CIN 3:
- Before the procedure: optimal preparation. We help make your immune system as strong as possible before the surgery. A well-functioning immune system promotes recovery after the procedure and helps in clearing any remaining HPV virus.
- After the procedure: addressing HPV. This is where our role is most important. After a LEEP procedure, the HPV virus is still present in 15-23% of women. With HPV type 16 that is persistently present, the risk of recurrence is up to 94%. We support your body through immune system support, supplements, and potentially escharotic treatment, with the aim of helping your body address the virus. The check-ups with your gynecologist remain leading.
- Intensive monitoring. Through quantitative HPV tests (viral load) and imaging, we monitor whether the virus is actually disappearing. This offers more insight than just the standard follow-up smear test after 6 months.
- Guidance and support. CIN 3 is a significant diagnosis. We take the time to answer all your questions and guide you through the entire process.
After LEEP procedure: HPV is not always gone
This is the point that surprises and frustrates many women. After a LEEP procedure, the abnormal cells have been removed, but the HPV virus can still be present in the surrounding tissue. The virus is not only in the abnormal cells, but also in seemingly healthy tissue around the treated zone.
The numbers speak for themselves:
- In 15-23% of LEEP procedures, the margins are not clear: abnormal cells are still present at the edge of the removed tissue.
- In women with persistent HPV type 16 after a LEEP procedure, the risk of recurrence (return of abnormal cells) is up to 94%.
- Even with clear margins, HPV can remain present and cause new abnormalities over time.
This is exactly why it is so important to keep paying attention to the HPV virus after a LEEP procedure. The surgery is the first step; supporting your body in addressing the virus can be a second step. HPV Health can support you with this, alongside the check-ups with your gynecologist.
recurrence risk with persistent HPV 16 after a LEEP procedure. Removing abnormal cells alone is not enough: the virus must also be addressed.
Bron: European Journal of Obstetrics & Gynecology
Had CIN 3? Ensure the HPV virus also disappears
After a LEEP procedure or conization, we help you actively clear the HPV virus and prevent recurrence. Schedule a consultation and discuss your options.
Schedule a consultationVeelgestelde vragen
Is CIN 3 cancer?
Can CIN 3 go away on its own?
How quickly does CIN 3 develop into cancer?
Can CIN 3 return after a LEEP procedure?
Can escharotic treatment be used for CIN 3?
Can I still have children after CIN 3 treatment?
Ready for the next step?
Schedule an intake and discover which holistic treatment suits you best.
Schedule an intake